By Lauren Ware
Whole-genome sequencing has the potential to help prevent or at least stifle outbreaks of infectious disease in hospitals, but it is by no means standard routine yet. Lauren Ware looks at the benefits and barriers to sequencing disease outbreaks.
Two months after the last patient infected with methicillin-resistant Staphylococcus aureus (MRSA) had been discharged from the special-care baby unit at a National Health Service Foundation Trust in Cambridge, UK, a team of researchers at the Wellcome Trust Sanger Institute in Cambridge, UK were analyzing samples from recent cases. They wanted to determine if these infections constituted an outbreak. Overall, the hospital’s data were ambiguous; there were gaps in the timeline of transmission of the cases of the disease that made it difficult to conclude if an outbreak had occurred over a six-month period. Then the hospital physicians contacted the team. A new case had popped up on the same ward.
The genomics team analyzed the new MRSA sample and confirmed that the new case was part of the original outbreak. Thanks to the high-resolution of current genome sequencing technology, the researchers could tell the hospital team that despite the gaps in the timeline of transmission, all the MRSA strains in the hospital were related. Furthermore, the data suggested it was an inside job, most likely a staff member acting as a MRSA infection carrier. So samples from 150 staff members were swabbed and sequenced. In a paper published in The Lancet: Infectious Diseases, the researchers reported that one healthcare worker was identified as the carrier (1). The worker was removed, treated, and then returned to work. Since then, there have been no further MRSA infections reported at the ward.
"It is very exciting," says Julian Parkhill, a microbiologist at the Sanger Institute. "This is the first time that genome sequencing has been used in real time to intervene in an outbreak. Without sequencing, that one new case would not have been sufficient to take action."
A few years from now, Parkhill imagines a future when DNA sequencing is routinely used in real time to get to the bottom of such outbreaks of multidrug-resistant bacteria. In this case, if sequencing had been used from the start, the outbreak could have been stopped six months earlier, when the first cases appeared. "For sequencing to be fully effective in infection control, this needs to be a routine tool. You need to spot the transmission events as they occur, not retrospectively," he says.
Changing Clinical Practice
For now, lower-resolution methods are used to identify bacteria in hospital settings, such as PCR assays that detect bacteria in specimens by identifying genes that confer antibiotic resistance. While multilocus sequence typing (MLST)—a typing method that looks at the sequence similarities between seven housekeeping genes—is sometimes used in the case of multidrug-resistant infections like MRSA, it's problematic because hospital-associated pathogens tend to be clonal; that is, most of them may be caused by bacteria belonging to the same sequence type. This level of resolution can't give clinicians the information they need to isolate the source of a cluster of infections. Plus, compared to requiring specific typing reagents for each different organism, sequencing is a single approach that can be used for all types of bacteria.
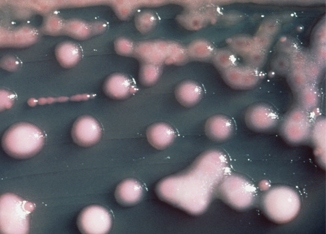
Genome sequencing could be particularly helpful for cases of Gram-negative multidrug-resistant bacteria, especially those resistant to the antibiotic carbapenem. In 2011, a cluster of carbapenem-resistant Klebsiella pneumoniae infections was discovered in the National Institutes of Health (NIH) Clinical Center (2). There, researchers used whole-genome sequencing to gain insight into the progression of the outbreak, creating a phylogenetic tree that showed that the infections were related to each other. This analysis revealed exactly how the bacteria had been transmitted between patients.
Even though sequencing is not yet standard, the information gleaned from studies using it has already changed clinical practice. "We learned that we need to be much more proactive in doing surveillance on patients, and we've been very honest about that because we don't want it to happen to anyone else," says Julia Segre, an investigator at the National Human Genome Research Institute in Bethesda, MD. The hospital has also begun to culture every patient who is transferred to the NIH Clinical Center from another hospital, to ensure they pick up any bacteria that might have been missed at their previous hospital.
Sharon Peacock, a clinical microbiologist at the University of Cambridge in the UK, says that sequencing could also be helpful for those with tuberculosis. Currently, it takes weeks or longer to complete full testing of tuberculosis for antibiotic resistance. Meanwhile, the patient must receive antibiotics without knowing if they are effective against his or her particular strain of tuberculosis. With sequencing, patients could be on an effective antibiotics regimen within a matter of days.
Why Isn't It Routine Already?
If genome sequencing can teach us so much about these types of hospital-acquired infections, why isn't it already being used routinely? Before this type of analysis can be made available at hospitals or even regional centers, the supporting infrastructure needs to be developed. The biggest hurdle is developing reference databases of bacterial genomes, something that shows what the population structure for a particular organism looks like.
"To analyze any one isolate, you need a database containing genomes to place it in genetic and geographic context," says Peacock. This would enable the analysis of newly sampled bacteria to be completed more quickly. Ideally, scientists would build an automated system that effectively encodes the expertise of the researchers currently doing the analysis. The clinicians would put in the sample, and they'd get a report with the sequence already analyzed into information they can use. "It's a hurdle," he says, "but it isn't a barrier. It is something that can be overcome."
Segre adds, "As a technical limitation, we also need those reference genomes sequenced with different instruments, which can cause slightly different results. We need to know what differences are due to the sequencing platform versus those due to the actual evolution of the bacteria."
While the recent studies using whole-genome sequencing to analyze the MRSA and Klebsiella outbreaks show that the technique is effective, the next step is to show that it is also cost-effective. "We have to get health economists and clinicians to start looking at cost," says Peacock. "This line of investigation hasn't been started yet."
Because bacteria have far fewer genes than humans, the cost of a whole-genome sequencing for those organisms is in the $100–200 range. But, of course, the costs of sequencing machines, data analysis, and the development of reference databases aren't counted in that figure. "We also need to do a detailed investigation of cost and benefit," says Peacock. "Where will this technology make a difference, and where will it not?"
In some cases, sequencing may indeed work just fine, she says, but it won't actually give you information that would change the course of illness. Saving sequencing for when it really matters can be key in terms of keeping costs reasonable. As far as the cost and turnaround of sequencing itself, "we don't have to do anything for that to go down," says Parkhill. "There is already a huge market for human genome sequencing, and that translates well to microbial sequencing."
References
Photo: In 2011, researchers used whole-genome sequencing to gain insight into the progression of a carbapenem-resistant Klebsiella pneumoniae outbreak at the National Institutes of Health (NIH) Clinical Center. Source: CDC

AtCDF3 gene induced greater production of sugars a...

Un estudio con datos de los últimos 35 años, ind...
Un equipo de investigadores de la Universidad Juli...

En nuestro post hablamos sobre este interesante tipo de célula del...
Palobiofarma S.L. is pleased to announce the “last patient last visi...










